What is MACS (Mild Autonomous Cortisol Secretion)? Top 8 Things You Need to Know

It is very important to highlight Mild Autonomous Cortisol Secretion (MACS) during Adrenal Awareness Month.
Mild Autonomous Cortisol Secretion (MACS) is a condition where the body produces excess cortisol, a hormone crucial for various bodily functions. Other names for MACS are subclinical Cushing’s syndrome (SCS) and primary hypercortisolism. YES! They are all names for the same thing. The names describe when there is too much cortisol from an adrenal tumor (or tumors, since bilateral disease occurs in about 20-30 %). We distinguish MACS and subclinical Cushing’s syndrome from severe, overt Cushing’s syndrome, when the cortisol levels are super high and you develop symptoms very rapidly often from an adrenal cancer or a pituitary tumor (Cushing’s disease).
So, what is MACS? Top 8 Things You Need to Know!
While it might not manifest severe symptoms initially, the long-term effects of MACS (subclinical Cushing’s syndrome) can impact health significantly. In this popular science piece, we delve into MACS, highlighting its definition, symptoms, and available treatments.
1) Understanding Mild Autonomous Cortisol Secretion: Definition and Mechanism
- MACS is characterized by the overproduction of cortisol by the adrenal glands, located on top of each kidney. This overproduction occurs independently of the body's normal regulatory mechanisms usually via a tumor, or multiple tumors on both adrenal glands (sometime mislabeled as “hyperplasia”), leading to elevated cortisol levels even when they are not required.
- Cortisol plays a vital role in regulating metabolism, immune response, and stress management. However, excessive cortisol levels can disrupt these functions, leading to various health issues.
2) Symptoms of Mild Autonomous Cortisol Secretion
- MACS often presents subtle symptoms that may go unnoticed initially. Common symptoms include weight gain, particularly around the abdomen, thinning of the skin, easy bruising, muscle weakness, fatigue, elevated glucose (pre- or frank diabetes) and high blood pressure.
- Individuals with MACS might also experience mood swings, irritability, anxiety, and depression due to the hormonal imbalance caused by excess cortisol.
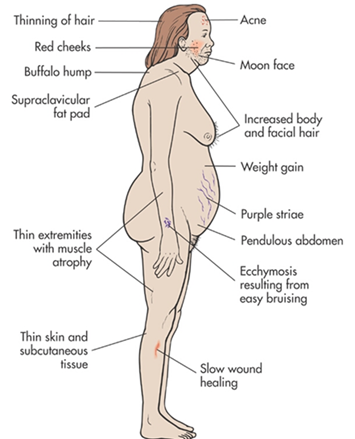
Figure 1. Common symptoms of Mild Autonomous Cortisol Secretion. Remember that cortisol is a toxic hormone and affects every cell of the body, so symptoms can be very individual and variable.
3) Diagnosis of Mild Autonomous Cortisol Secretion:
- Diagnosing MACS can be challenging because its symptoms overlap with those of other conditions like Cushing's syndrome.
- It should not be difficult to diagnose MACS, but many doctors have difficulty with this. There are three main test you need to run to assess cortisol production
- ACTH = Low to low-normal. The elevated cortisol from the adrenal tumor provides negative feedback to the pituitary which lowers the ACTH levels. If you have high ACTH levels, you do not have MACS, you may have a pituitary tumor causing Cushing’ syndrome.
- Low dose (1mg) dexamethasone suppression test (LDDST) = high, i.e. above 1.8 μg/dl. 1 mg of dexamethasone (a natural hormone; glucocorticoid; your endocrinologist will provide you a prescription for this) is given at 11 pm in the overnight test and the serum cortisol is measured the next day at 8-9 am (simple blood test). A normal person will “suppress” their cortisol to below 1.8 μg/dl. Patients with MACS fail to suppress and thus will have a cortisol level above 1.8 μg/dl.
- DHEA-S (Dehydroepiandrosterone-sulfate) = Low to low-normal, often below 100 μg/dl.
- Please note that 24-hour urinary free cortisol (UFC) and salivary cortisol levels are often measured by doctors. These are good tests for SEVERE Cushing’ syndrome but are normal in 95% of patients with MACS. Every week we see patients who have been told they cannot possibly have adrenal Cushing’s syndrome or MACS because their urine cortisol tests are normal. They have received erroneous information! Most patients with MACS will have normal 24h-UFC.
- Additionally, imaging studies such as MRI or CT scans should always be conducted to assess the adrenal glands and rule out other underlying causes. As you know, the best first imaging study is an adrenal-protocol CT scan.
4) Health Risks Associated with Mild Autonomous Cortisol Secretion:
- Long-term exposure to elevated cortisol levels can pose serious health risks. These include an increased risk of developing type 2 diabetes, osteoporosis, cardiovascular diseases such as hypertension and atherosclerosis, and compromised immune function.
- MACS can also have detrimental effects on mental health, leading to conditions like anxiety disorders and depression.
5) Medical Treatment Options for Mild Autonomous Cortisol Secretion:
- The primary goal of medical treatment for MACS is to normalize cortisol levels and alleviate symptoms, in the short term, and get the patients ready for surgery. This often involves the use of medications such as cortisol-lowering drugs like ketoconazole, metyrapone, or mifepristone. Some patients may need to lose significant weight prior to adrenal surgery and thus, need the above medications to help lose weight, and sometimes start GLP-1 agonist medications (Ozempic, etc).
- These medications work by inhibiting cortisol production or blocking its action in the body, thereby restoring hormonal balance. However, they may have side effects and require careful monitoring by healthcare professionals.
6) Surgical Treatment is the only cure for Mild Autonomous Cortisol Secretion:
- The only curative treatment is surgery, removing the adrenal tumor(s)
- Adrenalectomy, the surgical removal of one or both adrenal glands, is recommended to eliminate the source of excess cortisol production. This procedure provides a permanent cure for MACS.
- The best surgical option for almost all patients with MACS is the Mini Back Scope Adrenalectomy.
- For patients who have tumors on both adrenal glands, partial adrenalectomy (leaving a total of 30-50% of a normal adrenal gland) is often the best option to cure the MACS and at the same to avoid adrenal insufficiency.
7) Lifestyle Modifications for Managing Mild Autonomous Cortisol Secretion:
- Alongside medical or surgical interventions, lifestyle modifications can play a crucial role in managing MACS and reducing its impact on overall health.
- These may include adopting a healthy diet rich in fruits, vegetables, and whole grains while limiting processed foods and sugars. Regular exercise can also help in maintaining a healthy weight.
- Stress management techniques such as mindfulness and meditation can be beneficial in mitigating the effects of excess cortisol on mental well-being.
8) Long-Term Outlook and Prognosis of Mild Autonomous Cortisol Secretion:
- With proper diagnosis and management, the prognosis for individuals with MACS can be favorable. Surgical treatment can effectively control cortisol levels and alleviate symptoms, improving overall quality of life.
- However, long-term monitoring is essential to detect improvement in symptoms following surgery, as well as adjusting blood pressure and diabetes medications, since the glucose and blood pressure levels tend to improve after surgery. Also, weight loss after adrenal surgery should be monitored as well as regular laboratory studies, such as blood lipids (tend to improve after surgery). Regular follow-ups with healthcare providers can ensure timely adjustments to treatment plans and early intervention if necessary.
Conclusion:
Mild Autonomous Cortisol Secretion (MACS) presents a complex interplay of hormonal imbalance in the body, with far-reaching effects on physical and mental health. By understanding its definition, symptoms, and available treatment options, individuals affected by MACS can take proactive steps towards managing the condition effectively and leading a healthier life. Early diagnosis and intervention are key to minimizing the potential health risks associated with MACS and improving long-term outcomes.
Read more here: https://www.adrenal.com/blog/subclinical-cushings-syndrome-treatment-and-surgery
Additional Resources:
- Learn more about the Carling Adrenal Center
- Learn more about Dr. Tobias Carling
- Learn more about our sister surgeons at the Norman Parathyroid Center, Clayman Thyroid Center and Scarless Thyroid Surgery Center
- Learn more about the Hospital for Endocrine Surgery