New Important Research on Primary Aldosteronism and Cushing Syndrome

New Important Research on Primary Aldosteronism and Cushing Syndrome
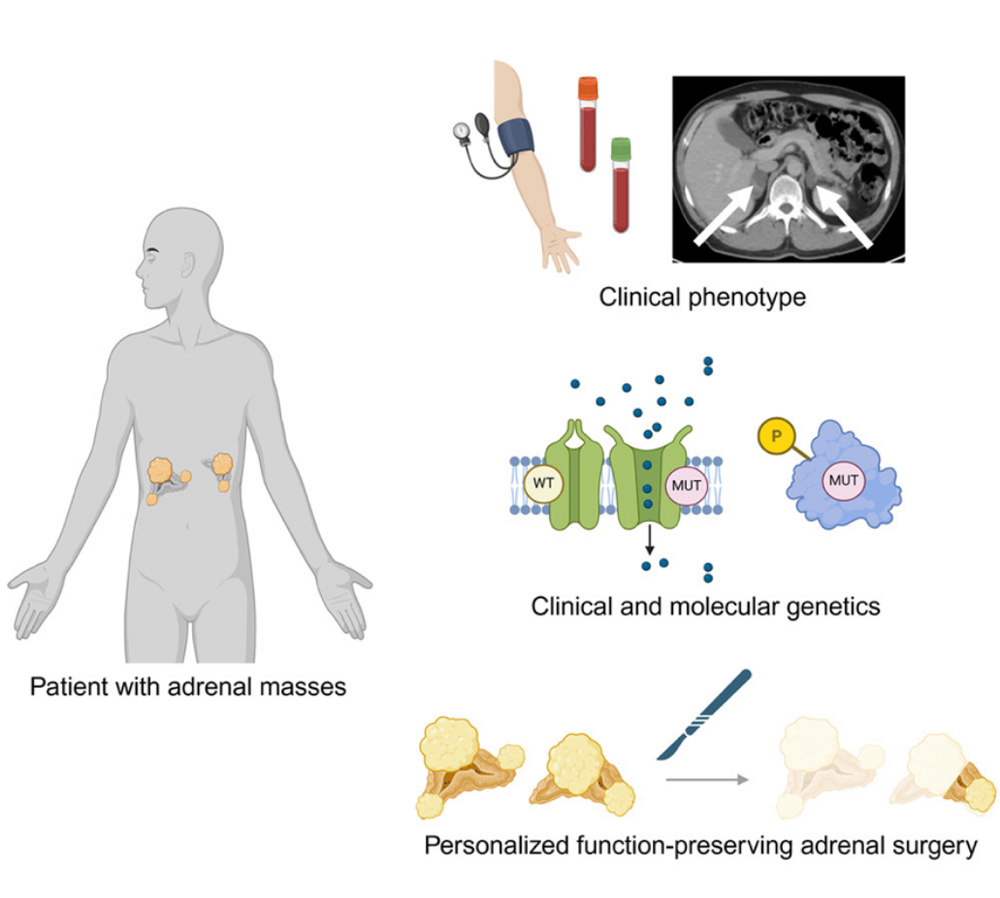
As a surgeon specializing in adrenal disorders at the Carling Adrenal Center, I am committed to advancing the understanding and treatment of conditions affecting the adrenal glands. These small organs, located atop the kidneys, play a critical role in hormone regulation, including aldosterone and cortisol. In our recent scientific article published in iScience (February 2026), titled "Molecular Pathology of Primary Aldosteronism and Hypercortisolism: Impact on Adrenal Surgery," my colleagues and I, Drs. Constantine A. Stratakis, Fabio R. Faucz, and C. Christofer Juhlin examine the latest molecular insights and their implications for surgical practice. This article highlights how these advancements are transforming patient care, particularly through precision surgery that minimizes risks and preserves adrenal function. While the molecular foundations are essential, our focus here emphasizes the evolving role of surgical interventions in improving outcomes for primary aldosteronism (PA) and adrenal hypercortisolism (AHC; adrenal Cushing syndrome).
Primary aldosteronism is the most common cause of secondary hypertension, resulting from excessive aldosterone production by the adrenal cortex. This leads to high blood pressure, hypokalemia, and increased risks of cardiovascular events such as stroke and heart failure. Despite its prevalence, affecting up to 10% of hypertensive individuals, fewer than 1% of cases are diagnosed and treated appropriately. Similarly, AHC involves autonomous cortisol overproduction from benign adrenal lesions, manifesting as overt Cushing syndrome with symptoms like central obesity, osteoporosis, diabetes, and psychiatric issues, or in milder forms known as mild autonomous cortisol secretion (MACS), which still contributes to significant morbidity and mortality. Surgical resection remains the definitive cure for both conditions, yet underdiagnosis and limited access to specialized care persist as major barriers.
Recent molecular studies have clarified the genetic drivers of these disorders, primarily involving mutations in ion channels for PA and the cAMP/PKA pathway for AHC. For PA, somatic mutations in genes like KCNJ5, CACNA1D, and ATP1A1 disrupt cellular signaling, leading to unchecked aldosterone synthesis. In AHC, alterations in PRKACA and ARMC5 are common, promoting cortisol excess. Epigenetic factors, such as DNA methylation and microRNA dysregulation, further influence disease presentation, particularly in diffuse or bilateral cases. These findings enable better pathological classification using tools like CYP11B2 immunohistochemistry and the HISTALDO algorithm, which distinguish classic adenomas from non-classic hyperplasia and inform prognosis. However, the true clinical impact lies in how this knowledge guides surgical strategies, shifting from total adrenalectomy to function-preserving approaches that reduce the lifelong burden of adrenal insufficiency.
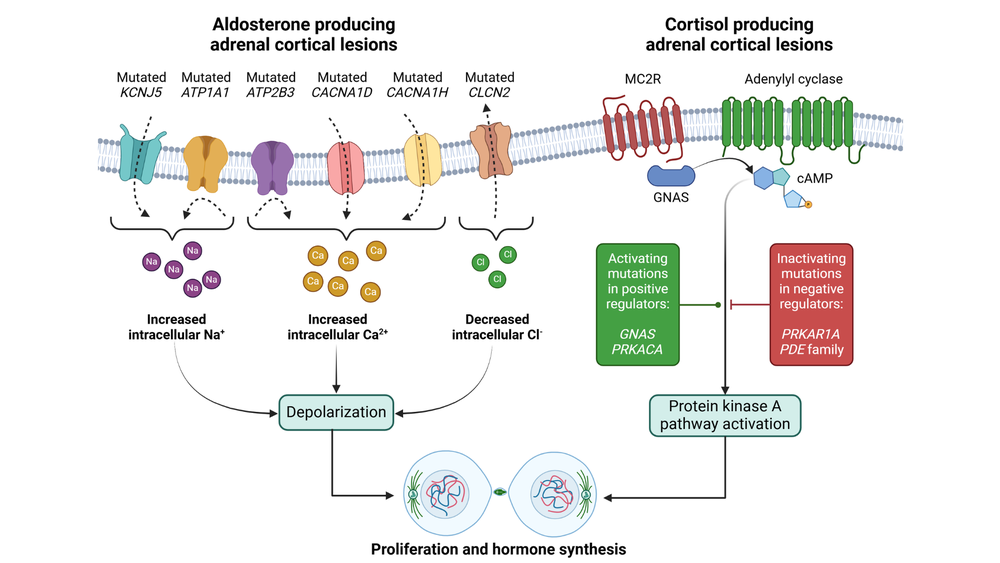
Figure 1: Summary of the genetic changes causing primary aldosteronism (PA) and adrenal hypercortisolism (AHC; adrenal Cushing syndrome).
The evolution of adrenal surgery has been marked by minimally invasive techniques, with mini back scope adrenalectomy (MBSA), also known as posterior retroperitoneoscopic adrenalectomy, emerging as a preferred method at high-volume centers. MBSA offers direct access to the adrenals through small flank incisions, minimizing tissue disruption, reducing operative time, and facilitating faster recovery with lower complication rates compared to transabdominal laparoscopic or robotic approaches. Critically, MBSA is ideally suited for function-preserving adrenalectomy, where only the hormone-producing lesions are excised, leaving at least 30% of healthy adrenal tissue in one gland (or 15% bilaterally) to maintain normal cortisol. Animal models and human studies confirm that this remnant size suffices to prevent hypocortisolism, avoiding the need for glucocorticoid replacement.
For PA, preoperative subtype classification is key to tailoring surgery. Cross-sectional imaging (CSI), such as CT or MRI, identifies unilateral adenomas (APAs >1 cm), nodules (APNs <1 cm), or micronodules (APMs), which may be multifocal or bilateral. Adrenal vein sampling (AVS) lateralizes aldosterone excess but is invasive, technically demanding, and often unavailable or unsuccessful, leading to undertreatment. Our review advocates an individualized AVS approach, considering patient factors like age, biochemical severity, and access to expertise. With function-preserving options, AVS becomes less pivotal, as bilateral disease can be addressed without risking insufficiency.
For unilateral PA, partial resection cures most cases with excellent biochemical and clinical outcomes, resolving hypokalemia and improving hypertension. In bilateral PA, often milder but associated with persistent morbidity, evidence supports unilateral or staged bilateral partial adrenalectomy over medical therapy alone. Staged procedures, spaced at least six weeks apart, allow assessment of postoperative outcomes using PASO (internationally accepted definition of surgery outcomes) criteria, pathology, and genetics, determining if contralateral intervention is needed. This minimizes unnecessary operations and adrenal insufficiency risks. Genotype-phenotype correlations, such as KCNJ5 mutations predicting favorable results, further refine patient selection.
In AHC, similar principles apply. Subtypes include unilateral cortisol-producing adenomas (CPAs), bilateral macronodular disease (BMAD), or micronodular disease (BMiNAD), often with germline mutations. Overt Cushing warrants surgery, while the benefit in mild AHC (MACS) patients is increasingly recognized, as a recent trial showed superior hypertension reversal with adrenalectomy versus medication. Patients also improve in quality of life, glucose intolerance, diabetes control, bone loss, etc., with reduced risk of cardiovascular morbidity and mortality after surgery. Staged bilateral function-preserving adrenalectomy achieves 92–98% cure rates with low recurrence and steroid needs. One study comparing partial versus total unilateral adrenalectomy in 141 cases found shorter corticosteroid therapy duration (4% vs. 25% requiring >2 years) with partial approaches. AVS may guide laterality in bilateral cases when total removal is planned, but we favor bilateral preservation to avoid insufficiency.
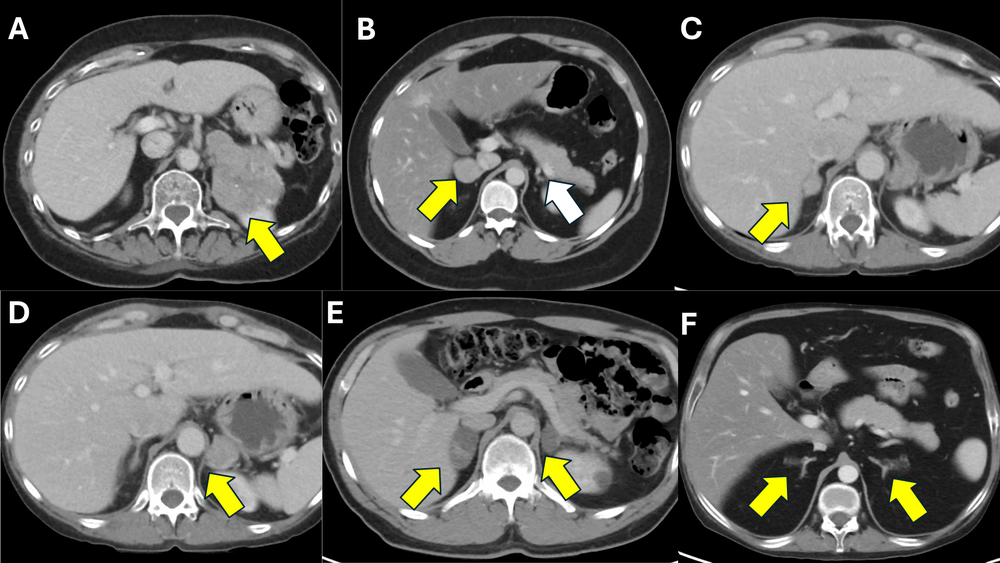
Figure 2: Representative CT scan images from patients with various subtypes of cortisol-producing adrenal lesions causing ACTH-independent Cushing’s syndrome.
A) A 70-year-old female with a large left adrenocortical carcinoma (ACC; yellow arrow), causing severe, overt adrenal Cushing’s syndrome.
B) A 25-year-old female with a right adrenocortical adenoma (yellow arrow), causing overt adrenal Cushing syndrome (CPA), with a suppressed, atrophic right adrenal gland (white arrow).
C and D) A 43-year-old female with bilateral CPAs (yellow arrows), causing overt adrenal Cushing syndrome.
E) A 49-year-old male with a bilateral macronodular adrenocortical disease (BMAD) (yellow arrows), causing subclinical Cushing syndrome (mild autonomous cortisol secretion; MACS).
F) A 31-year-old male with a bilateral micronodular adrenocortical disease (BMiNAD) (yellow arrows), causing severe, overt adrenal Cushing syndrome, in the setting of primary pigmented nodular adrenocortical disease (PPNAD).
Postoperative management is crucial. For PA, biochemical cure is assessed via aldosterone-renin ratios; for AHC, cosyntropin stimulation tests identify insufficiency risks, guiding transient steroid use. Long-term follow-up monitors recurrence, especially in non-classic histology or germline-mutated cases. These advancements promise broader adrenalectomy indications, saving lives by addressing undertreated morbidity.
In summary, our article underscores a paradigm shift toward precision, function-preserving adrenalectomy, enhancing safety and efficacy. At specialized centers, this approach expands curative options, even for complex bilateral disease. Patients with resistant hypertension or cortisol-related symptoms should seek evaluation—early intervention can profoundly improve quality of life.
For further discussion, consult the full article at https://doi.org/10.1016/j.isci.2026.114910.
- Carling T, Stratakis CA, Faucz FR, Juhlin CC. Molecular pathology of primary aldosteronism and hypercortisolism: Impact on adrenal surgery. iScience. 2026 Feb 5;29(3):114910. doi: 10.1016/j.isci.2026.114910. PMID: 41736857
Have questions? Reach out to us at the Carling Adrenal Center. We’re here to help you get answers and get back to living your best life.
Dr. Tobias Carling, of the Carling Adrenal Center, is one of the world's leading experts in adrenal gland surgery. Dr. Carling performs more adrenal operations than any other surgeon in America. Dr. Carling left Yale University in 2020 to open the Carling Adrenal Center in Tampa, Florida.
To discuss the details of your case with Dr. Carling and become his patient, fill out the new patient form, and he will be in touch with you shortly.
Additional Resources:
- Learn more about the Carling Adrenal Center
- Learn more about Dr. Tobias Carling
- Learn more about our sister surgeons at the Norman Parathyroid Center and Clayman Thyroid Center.
- Learn more about the Hospital for Endocrine Surgery