New Important Pheochromocytoma Research Published by Dr. Carling and the Carling Adrenal Center

New Important Pheochromocytoma Research Published by Dr. Carling and the Carling Adrenal Center
Pheochromocytomas are tumors that develop in the adrenal glands, small hormone-producing organs sitting atop your kidneys. These tumors often release excess adrenaline and similar hormones, causing dramatic symptoms like sudden high blood pressure, severe headaches, rapid heartbeat, and heavy sweating. But not all of them act this way. A growing number present quietly, without any classic warning signs, and that's what makes silent pheochromocytoma so challenging to spot.
Recent research from the Carling Adrenal Center, the highest volume adrenal surgery hospital (currently performing >650 adrenal operations per year) in the world, published in Endocrine Practice in 2025, highlights the clinical features of silent pheochromocytoma and underscores its underrecognized prevalence.
.png?x=9.66&y=64.88215488215488&w=538.1999999999999&h=277.47474747474746)
Study Overview
Over nearly three years (2022–2024), Dr. Carling and the Hospital for Endocrine Surgery performed close to 1,300 adrenal operations and found 103 confirmed pheochromocytomas. After excluding hereditary (genetic) cases, about 15% (14 out of 94 sporadic tumors) were silent: no typical symptoms and only mildly elevated (or normal) hormone levels in the blood or urine.
These silent tumors were smaller, averaging just under 3 cm in diameter compared to 4.5 cm for the symptomatic ones, and their hormone output was much lower, often only slightly above normal limits. This subtlety explains why they fly under the radar.
Why Silent Pheochromocytomas Are Often Missed
One of the biggest issues is imaging. When these tumors are discovered incidentally (during scans for something else), outside radiologists frequently mislabel them:
- As harmless, benign adenomas (fatty tumors that sometimes don't need treatment)
- As "indeterminate" or atypical lesions
- Rarely, as possible cancer spread from somewhere else
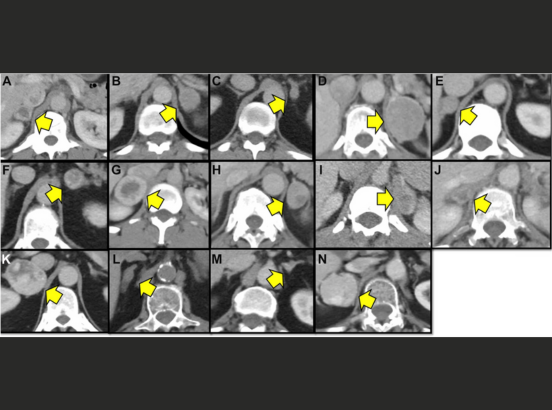
In the study, standard CT scans showed these tumors had higher density (often 20–37 Hounsfield units) than typical adenomas, but reports sometimes overlooked this key detail. Specialized "adrenal protocol" scans with multiple phases of contrast can help clarify, yet they're not always used at other hospitals.
Adding to the confusion, over 40% of these silent cases also showed mild excess cortisol (adrenal hypercortisolism, Cushing syndrome) production from the adrenal cortex—the outer layer of the gland. This overlap can lead doctors to focus on cortisol issues and miss the pheochromocytoma.
Patients came from across the U.S. and internationally (60%), with many traveling long distances for expert surgery by Dr. Carling—highlighting how specialized centers attract complex cases. About 40% of the patients came from Florida (in-state).
.png)
Figure 1: Adrenal protocol CT scans of 14 pheochromocytoma patients, showing pheochromocytomas (yellow arrows) often misinterpreted by other hospitals as adenomas, atypical lesions, or possible metastases.
Safe and Effective Treatment
The good news? Surgery cures these tumors, and outcomes are excellent, especially with modern minimally invasive techniques. The Carling Adrenal Center used the MBSA (Mini Back Scope Adrenalectomy) approach (posterior retroperitoneoscopic adrenalectomy) in all cases, which is the best operation for adrenal tumor removal. This involves small incisions in the back, direct access to the adrenal, shorter operating times (often under 20 minutes), minimal pain, and discharge the very next morning.
What This Means for Patients and Doctors
Silent pheochromocytoma isn't as rare as once thought, especially in centers seeing tough adrenal cases. Left undiagnosed, even quiet tumors carry risks: a sudden hormone surge during stress or unrelated procedures, or (very rarely) spread. The key to catching them early lies in:
- Routine blood tests for metanephrines (the most reliable marker) whenever an adrenal mass is found
- Better imaging protocols
- A higher index of suspicion, especially for smaller tumors or those with mild hormone changes
If you or someone you know has an adrenal "incidentaloma", don't settle for a quick dismissal. Push for complete hormone testing and, if needed, evaluation at an experienced center. Catching a silent pheochromocytoma early turns a potential hidden threat into a straightforward, curable condition.
Reference:
- LaRue M, Stratakis CA, Kalik A, Faucz FR, Carling T. Silent Pheochromocytoma is an Underrecognized Clinical Entity: Results from a High-Volume Adrenal Surgery Hospital. Endocr Pract. 2025 Dec 17:S1530-891X(25)01325-4. doi: 10.1016/j.eprac.2025.12.005. Epub ahead of print. PMID: 4141918
Dr. Tobias Carling, of the Carling Adrenal Center, is one of the world's leading experts in adrenal gland surgery. Dr. Carling performs more adrenal operations than any other surgeon in America. Dr. Carling left Yale University in 2020 to open the Carling Adrenal Center in Tampa, Florida.
To discuss the details of your case with Dr. Carling and become his patient, fill out the new patient form and he will be in touch with you shortly.
Additional Resources:
- Learn more about the Carling Adrenal Center
- Learn more about Dr. Tobias Carling
- Learn more about our sister surgeons at the Norman Parathyroid Center, and Clayman Thyroid Center.
- Learn more about the Hospital for Endocrine Surgery