What are the Symptoms of Pheochromocytomas?
 Signs and symptoms of Pheochromocytoma and Paraganglioma. The symptoms can be very variable, and some patients are asymptomatic.
Signs and symptoms of Pheochromocytoma and Paraganglioma. The symptoms can be very variable, and some patients are asymptomatic.
The classic symptoms of pheochromocytomas (or pheos) are those symptoms that are caused by the excess adrenaline being produced within the adrenal gland tumor. The list below shows the classic symptoms, but some patients have no symptoms at times, and only have symptoms on occasion. Also, pheochromocytomas have been called the great “mimicker” because the symptoms of pheochromocytomas can mimic those of many other diseases. Nonetheless, the patients that do have symptoms from their pheo are often characterized by paroxysms (they have “spells” of symptoms), and at other times feel just fine.
This List Summarizes a Typical Paroxysm “Spell” of Symptoms From a Pheochromocytoma
- Headache, sweating, and palpitations
- Very high BP (frequently with tachycardia)
- Chest or abdominal pain
- Pallor/flush
- Apprehension (sense of impending doom)
- Duration (5 min to an hour or longer)
- Spells may be spontaneous or precipitated by change in body position, anxiety, medications (e.g., metoclopramide, anesthetic agents), and maneuvers that increase intraabdominal pressure (e.g. going to the bathroom).
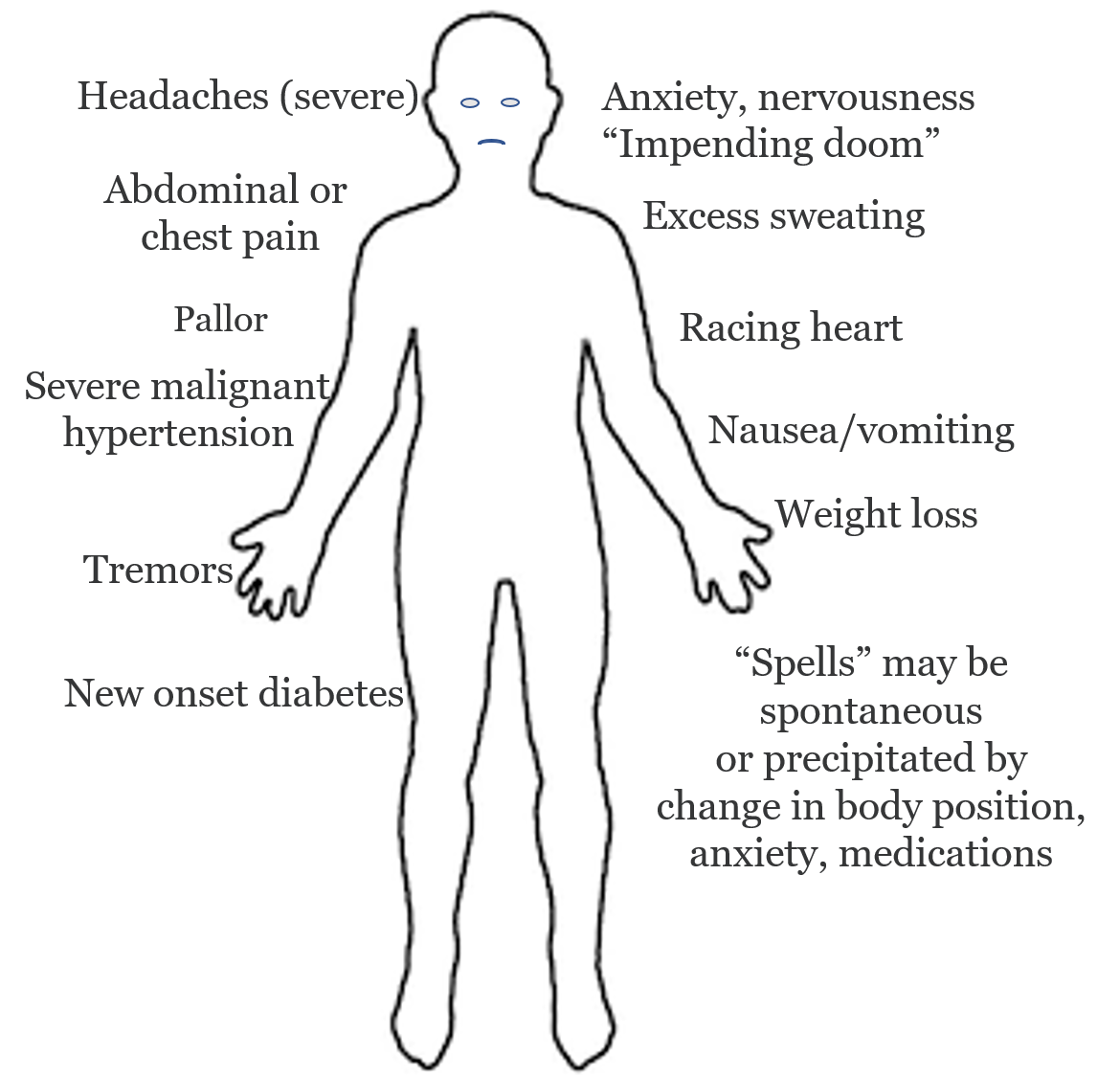
Other Typical Signs and Symptoms of Pheochrmocytoma Include:
- Headaches (severe)
- Excess sweating (generalized)
- Racing heart (tachycardia and palpitations)
- Anxiety and nervousness
- Nervous shaking (tremors)
- Pain in the lower chest or upper abdomen
- Nausea (with or without vomiting)
- Weight loss
- Heat intolerance
- Weight loss
- Recent onset of hypertension
- Severe or malignant hypertension
- Tachycardia (occasional racing heart)
- Marked blood pressure lability
- Carbohydrate intolerance or overt new onset diabetes mellitus
- Adrenal mass on imaging
- Orthostatic hypotension in untreated state (get faint when you stand up)
- Family history of pheochromocytoma
- Unanticipated prominent changes in BP (up or down) in response to drugs or diagnostic manipulations
Read more about symptoms of pheochromocytoma on our adrenal surgery blog
Complications and Quality-of-life issues with Untreated Pheochromocytoma
Why are pheochromocytomas (and paragangliomas), so important, and why are we so eager to get patients treated? This has to do with the extremely toxic effects of too high adrenaline type hormone levels (this is called Target Organ Damage). It is also important because only a fraction of all patients (< 10%) are being diagnosed, and not all patients are being offered surgery. It is estimated that about 5 % of patients with an adrenal mass, have pheochromocytoma. This toxic (and very silent) disease can often be cured by a 20-30-minute operation. This is what we do, and unfortunately, it is common that patients by the time they see Dr. Carling have had symptoms for years to decades. The toxic effects of too much adrenaline type hormones affects your entire body, especially the heart, blood vessels, kidney, and central nervous system (CNS; brain)High blood pressure is the most common clinical feature of pheochromocytoma. The traditional estimate is that 90% of pheochromocytoma patients are hypertensive; the normotensive ones are found incidentally during imaging for an unrelated problem or during the process of family screening in kindreds with syndromic pheochromocytomas. It is worth emphasizing that with increasing recognition of familial pheochromocytoma and paraganglioma, those cases found by screening will likely increase.
High blood pressure in pheochromocytomas and paragangliomas • Sustained 60% • With crises 27% • Without crises 33% • Paroxysmal 30% (Normal blood pressure between attacks) • No hypertension 10% (Discovered incidentally or through screening)
It is noteworthy that more than one-half of pheochromocytoma and paraganglioma, patients do not have discrete spells. This is the group that masquerades as essential hypertension. The high blood pressure whether sustained or episodic puts the patient at great risk of a stroke.
Chest pain may reflect poor blood flow to the heart (cardiac ischemia) from either an increase in demand or a decrease in supply of blood and oxygen to the heart. This puts you at risk of heart damage (heart attacks, heart arrhythmias, and sudden death).
Congestive heart failure in patients with pheochromocytomas and paragangliomas may occur because of dysfunction due to adrenaline type hormones causing cardiac hypertrophy (the heart grows too big, and ineffective).
Abdominal pain, which may be associated with nausea and vomiting, often reflects hemorrhagic infarction within the tumor (the pheochromocytomas and paragangliomas can spontaneously start to bleed). Gallstones are also more common in these patients and may cause pain on the right side of the upper abdomen.
Sweating reflects the increase in heat production stimulated by adrenaline type hormones.
Weight loss in pheochromocytomas and paragangliomas patients is another consequence of the increased metabolic rate due to adrenaline type hormones.
Orthostatic hypotension (medical term for that your blood pressure drops when you stand up; often causing dizziness) is an important manifestation of pheochromocytomas and paragangliomas. In fact, in an untreated hypertensive patient, a prominent fall in BP on standing (20/10 mmHg) should raise the suspicion of pheochromocytoma.
Rhabdomyolysis (break down of your muscles) and ischemic colitis (your large bowel may not get enough blood and in worst case die) are rare complications of pheochromocytomas and paragangliomas secondary to intense vasoconstriction in the skeletal muscle and colon, respectively.
Hypotension or shock is infrequent but important manifestations of pheochromocytomas and paragangliomas since they may be associated with significant morbidity or death.
Acute respiratory distress syndrome (ARDS) or “shock lung” is a rare but serious complication of pheochromocytomas and paragangliomas. In some cases it is the presenting manifestation; in others it develops in the wake of a particularly severe paroxysm. It is frequently associated with hypotension, presumably due to the release of adrenaline typre hormones from the tumor.
Acute abdominal catastrophe is another infrequent but well-recognized presentation. It is associated with abdominal pain, frequently shock, but sometimes with high and/or fluctuating blood pressure. The cause is usually hemorrhage into the tumor, sometime with the extravasation of blood into the peritoneal space.
Become Our Patient
Patients needing adrenal surgery travel from all over the world to have adrenal surgery with Dr. Carling, the most experienced adrenal surgeon. This page discusses how you can have your adrenal operation at the Carling Adrenal Center with Dr. Carling himself.What to read next
- Surgery for pheochromocytomas - learn about the different types of surgery for pheos, and why one operation is prefered over others.
- Mini-Back-Scope-Surgery - the preferred adrenal operation for 95% of pheochromocytomas.
- More about our founder Dr Tobias Carling - the most experienced adrenal surgeon in the world.
- How to become our patient, and have Dr Carling perform your pheo operation.