What is the Best Scan for Adrenal Gland Tumor and Conn's Syndrome?
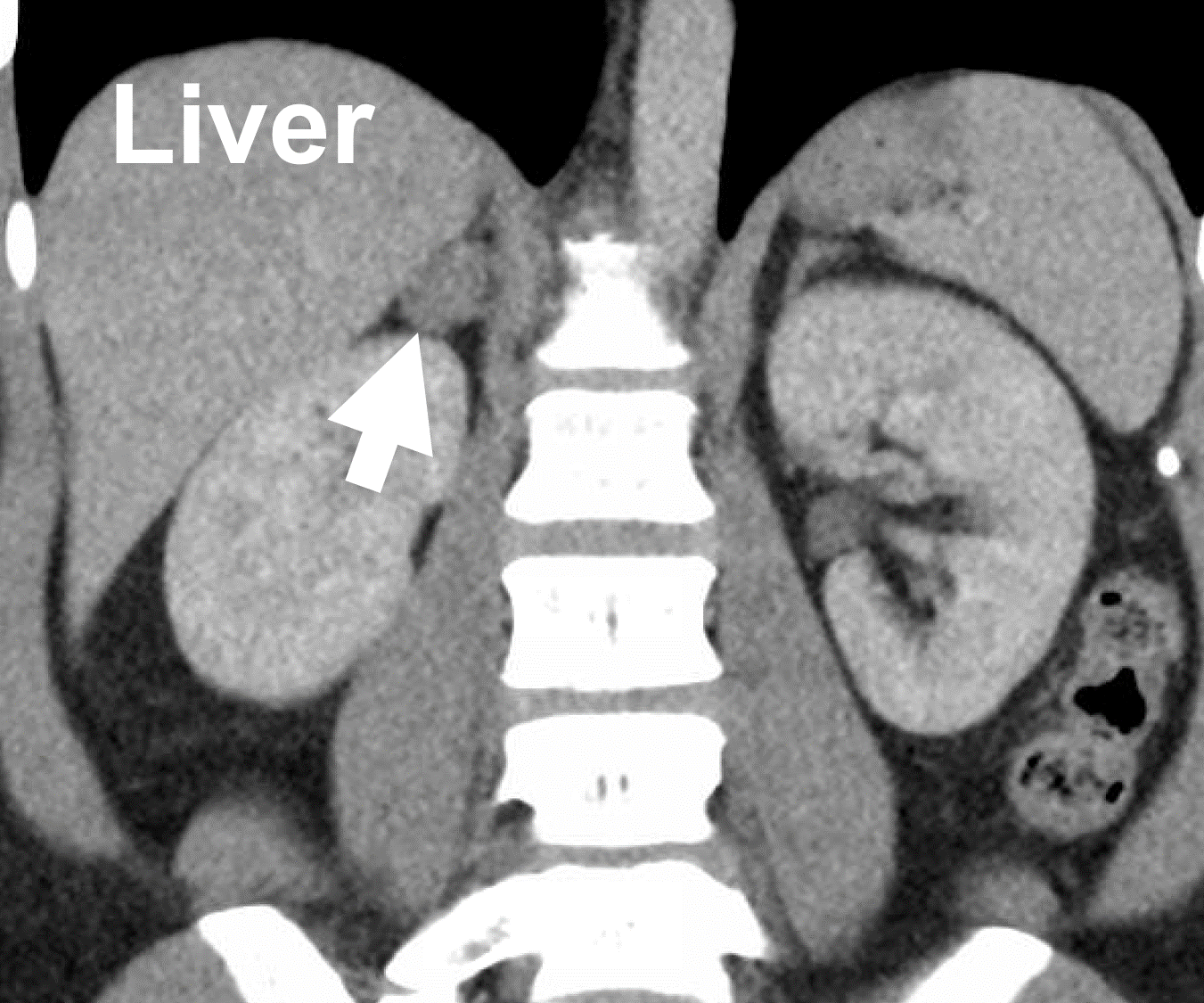 A typical CT scan demonstrating a right aldosterone-producing adrenal adenoma (arrow) causing Conn’ syndrome.
Without a doubt the best x-ray or scan for patients with primary hyperaldosteronism is a "contrast-enhanced CT scan”. On an unenhanced (no contrast) CT, adenomas are usually well-demarcated round or oval lesions, with homogeneous and relatively low attenuation values. The addition of contrast help visualize vessels better, and thus, having a CT scan with and without contrast is the best. If you are allergic to i.v. contrast, you can have a non-contrast CT scan, which is not as good, but better than no scan. In almost all cases, this scan is all you need. Only occasionally is an MRI helpful in these patients. Dr. Carling published one of the landmark research studies when it comes to imaging of aldosterone-producing adenoma (APA). We often refer to this type of CAT scan with contrast for the adrenal gland the adrenal-protocol CT scan.
A typical CT scan demonstrating a right aldosterone-producing adrenal adenoma (arrow) causing Conn’ syndrome.
Without a doubt the best x-ray or scan for patients with primary hyperaldosteronism is a "contrast-enhanced CT scan”. On an unenhanced (no contrast) CT, adenomas are usually well-demarcated round or oval lesions, with homogeneous and relatively low attenuation values. The addition of contrast help visualize vessels better, and thus, having a CT scan with and without contrast is the best. If you are allergic to i.v. contrast, you can have a non-contrast CT scan, which is not as good, but better than no scan. In almost all cases, this scan is all you need. Only occasionally is an MRI helpful in these patients. Dr. Carling published one of the landmark research studies when it comes to imaging of aldosterone-producing adenoma (APA). We often refer to this type of CAT scan with contrast for the adrenal gland the adrenal-protocol CT scan.
Dr. Carling’s very high volume of these operations has allowed him to publish scientific studies demonstrated that in aldosterone-producing adenomas (APA), there is a strong correlation between the imaging phenotype (i.e. what your tumor looks like on a CT scan), histology (what your tumor looks like under the microscope) and genotype (what gene is mutated in the tumor). This is important since he can then predict who can go straight to surgery with excellent outcomes, and who may need adrenal vein sampling.
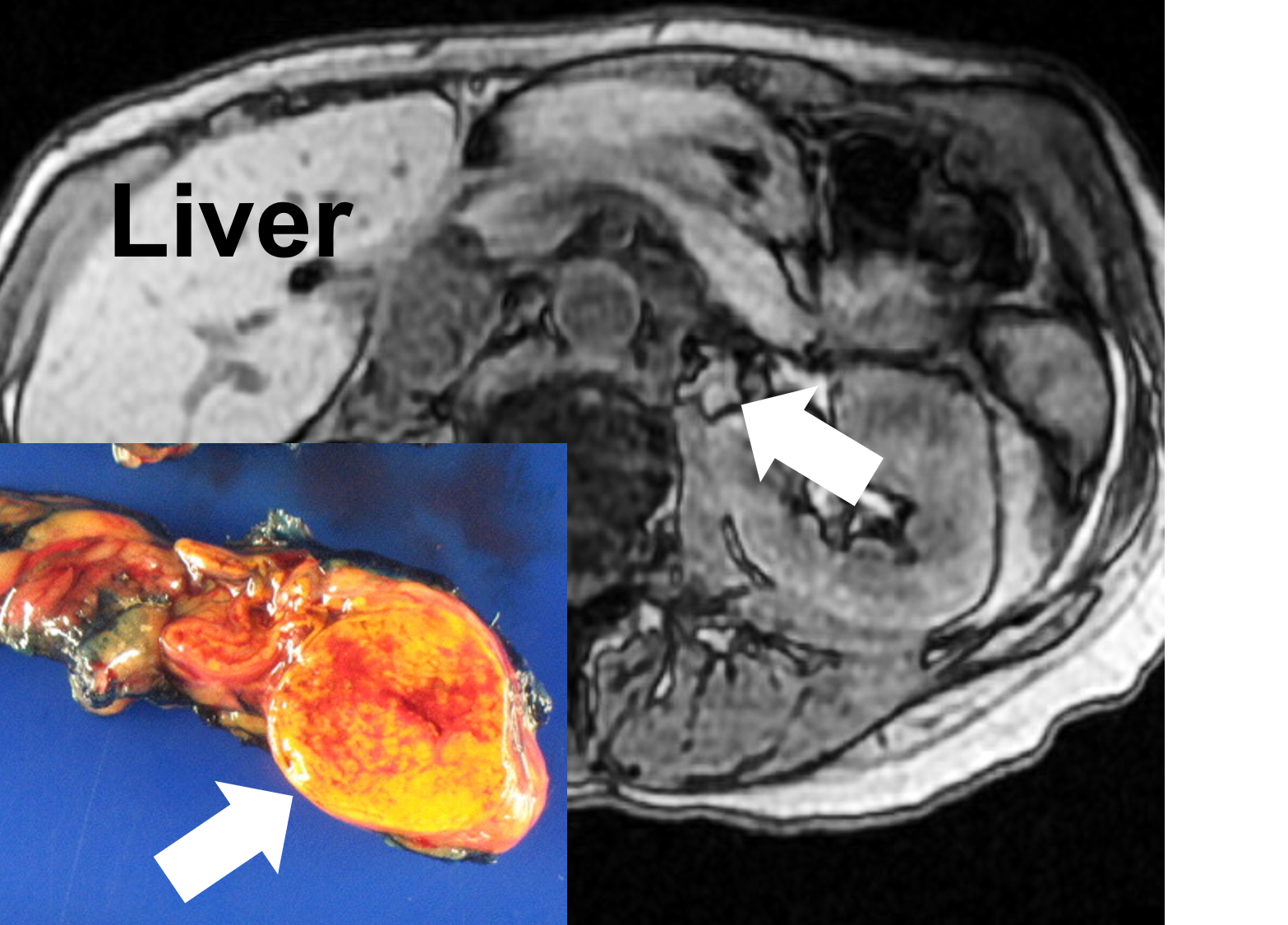 An MRI demonstrating a left aldosteronoma (arrow aldosterone-producing adenoma; APA) causing Conn’s syndrome, and after removal via Mini Back Scope Adrenalectomy (MBSA).
Dr. Carling, Editorial note: If you have primary hyperaldosteronism, do not worry what your endocrinologist or radiologist (X-ray) doctor thinks about your scan, your tumor size, or tumor location--let us decide--we do more of this than anybody. Also, do not waste time obtaining unnecessary expensive scans (for instance an MRI), or an invasive adrenal vein sampling procedure. In rare cases you may need it, but most often you don’t and inexperienced doctors and surgeons will get MANY scans and x-rays that you do not need. Dr. Carling has seen it all and almost all patients have scans they did not need and these scans confuse the doctors and give the patients and the doctors too much fear and apprehension. Dr. Carling has created the scientific basis of the disease via the major international studies and can in minutes figure out what is going on with your adrenal tumor, i.e. the aldosterone-producing adrenal adenoma (APA).
An MRI demonstrating a left aldosteronoma (arrow aldosterone-producing adenoma; APA) causing Conn’s syndrome, and after removal via Mini Back Scope Adrenalectomy (MBSA).
Dr. Carling, Editorial note: If you have primary hyperaldosteronism, do not worry what your endocrinologist or radiologist (X-ray) doctor thinks about your scan, your tumor size, or tumor location--let us decide--we do more of this than anybody. Also, do not waste time obtaining unnecessary expensive scans (for instance an MRI), or an invasive adrenal vein sampling procedure. In rare cases you may need it, but most often you don’t and inexperienced doctors and surgeons will get MANY scans and x-rays that you do not need. Dr. Carling has seen it all and almost all patients have scans they did not need and these scans confuse the doctors and give the patients and the doctors too much fear and apprehension. Dr. Carling has created the scientific basis of the disease via the major international studies and can in minutes figure out what is going on with your adrenal tumor, i.e. the aldosterone-producing adrenal adenoma (APA).
Adrenal Vein Sampling (AVS) for adrenal tumors. Adrenal vein sampling is sometimes needed to distinguish unilateral from bilateral adrenal sources of aldosterone secretion. This is an interventional radiology study. AVS should be performed in all patients with a CT scan that is equivocal or demonstrates adrenal tumors on both the right and the left side. Through small catheters blood samples are obtained from each adrenal vein and the inferior vena cava sequentially, or simultaneously. In experienced centers, the bilateral adrenal veins are catheterized and sampled with a technical success rate exceeding 90%. Technical success is directly associated with operator experience, leading to the recommendation that the procedure be performed by one or two operators at a institution to maximize expertise. Dr. Carling, Editorial note: Unless your endocrinologist has extensive experience in identifying the best interventional radiologist to perform the Adrenal Vein Sampling procedure (if you need it), call us! We know who can do this procedure with great success rates and safely. But remember, MANY patients with Conn's Syndrome and hyperaldosteronism do not need Adrenal Vein Sampling.
Warning: Technical Information about Adrenal Vein Sampling: Because the normal adrenal gland produces cortisol in response to ACTH, venous cortisol levels are used as a positive control to determine that the AV is adequately sampled. The cortisol level in each adrenal vein is compared to peripheral samples taken from the inferior vena cava. Once it has been proven that both left and right adrenal veins have been adequately sampled, the next step is to determine if results are lateralizing to one gland (see if the hormone is higher on one side than the other). The aldosterone level (A) in each sample is normalized to the cortisol level. Then, one side is divided by the other to determine the lateralization index (LI) A lateralization index greater than 4 is compatible with a unilateral source of aldosterone. Most centers use the LI to diagnose unilateral etiologies of PA; contralateral gland suppression can also confirm the presence of an aldosterone-producing adenomas (APA).
Dr. Carling, Editorial note: Again, if you have primary hyperaldosteronism, let us review your imaging (send us your CT scan). Dr. Carling has more experience looking at adrenal tumors on CT scans (and has published widely about it) than almost any endocrinologist or radiologist (X-ray) doctor in the world. Also, do not waste time obtaining unnecessary expensive scans (for instance an MRI that almost nobody with this type of adrenal problem needs), or an invasive adrenal vein sampling procedure. Occasionally you may need it, but most often you don’t. Dr. Carling has seen it all. He has created the scientific basis of the disease via the major international studies and can in minutes figure out provided what is going on with your aldosterone-producing adenomas (APA).
What are the top 10 Things to Know About Adrenal Vein Sampling for Primary Hyperaldosteronism (Conn's Syndrome)? Read more on our adrenal surgery blog
If you have an adrenal gland tumor, do not fret. This is all we do and we can make this very easy for you. Simply contact us. Send us your data and your scan. We know what to do. We can save you significant time and money avoiding wasteful and unnecessary test and get you on your way to a cure!
