Are Adrenal Tumors Common?
Adrenal tumors are common, occuring in 2-3% of adults in their lifetime. The most common adrenal problems are the developement of benign, non-cancerous tumors inside the adrenal gland. When you have a tumor of the adrenal gland, the first thing you need to figure out is whether it’s overproducing any adrenal hormones. These hormones are aldosterone, cortisol and catecholamines (also known as epinephrine and norepinephrine; adrenaline), and, more rarely, sex-steroid hormones (androgens and estrogens). A tumor that is overproducing any of these hormones is called a "functional" (or endocrine active) tumor. It is called a functional tumor because it is overfunctioning, i.e. overproducing hormones.
 A functional adrenal tumor producing excess aldosterone causing Conn's Syndrome.
A functional adrenal tumor producing excess aldosterone causing Conn's Syndrome.
Functional Adrenal Tumors are Common and Produe Too Much Hormones Making You Sick
Adrenal tumors that produce hormones are called "functional" adrenal tumors. That means they are functional as intended to produce hormones--but they just produce too much of the hormone. A tumor that is overproducing cortisol causes Cushing’s syndrome or subclinical Cushing’s syndrome. A tumor that is overproducing aldosterone causes primary hyperaldosteronism also known as an aldosteronoma or Conn's tumor. A tumor that is overproducing catecholamines (also known as epinephrine and norepinephrine; adrenaline) is called a pheochromocytoma.Most functional adrenal tumors are benign. It is important for you to understand that most functional adrenal tumors are benign (non-cancerous). That means, if your adrenal tumor produces too much cortisol, aldosterone or adrenaline-type hormones (catecholamines) it is almost always benign. In the picture above, the round tumor is easily seen within the triangle-shaped adrenal gland that Dr. Carling removed from a 38-year-old woman. The round tumor measured 1.5 cm (3/4 inch) in diameter and was producing too much aldosterone. This woman had high blood pressure and low potassium in her blood due to excess aldosterone production. This is called Conn's Syndrome. We operate on people with Conn's Syndrome and tumors like this several times per week. Most of these mini-scope operations (Mini Back Scope Adrenalectomy; MBSA) take Dr. Carling about 30 minutes and the patient has only a few small Band-Aids on their lower back.
 Typical small Band-Aids at the patients flank after a 23-minute Mini Back Scope Adrenalectomy; MBSA for a functional adrenal tumor causing Conn's Syndrome.
Typical small Band-Aids at the patients flank after a 23-minute Mini Back Scope Adrenalectomy; MBSA for a functional adrenal tumor causing Conn's Syndrome.
IMPORTANT: If the adrenal tumor has overproduction of sex-steroid hormones, this almost always occurs in the setting of a cancerous tumor, so is is very important to know which hormones are being produced by the adenal tumor.
Do Functioning Adrenal Tumors Need to be Removed?
Yes, anytime you have a functional tumor, it needs to be removed. Not primarily because of the concern for cancer, but the damage caused to the body due to excess of these "toxic" hormones. You need an adrenalectomy. You can learn more about adrenal surgery on other pages of this website. Dr. Carling is the world's leader in performing mini-surgery for functional adrenal tumors, performing this operation almost every day.Steps to Take to Determine Treatment of an Adrenal Tumor
The first step is always to figure out whether the adrenal tumor is functional or not. This is done by a very careful history and physical exam by an experienced doctor and then a combination of blood and urine laboratory tests. Even if the tumor is nonfunctional (there is no evidence that the tumor is over producing hormones) it still can be a potential problem.The second step is to determine if the tumor is really arising from the adrenal or is there something else going on in the vicinity of the adrenal gland? Thus he next question then is to figure out for sure if the tumor we see on CT scan is an adrenal gland tumor or something nearby. It could be a different kind of tumor that is just adjacent to the adrenal gland, but not arising from the adrenal gland. This is very important. Often radiological imaging is very helpful here. Dr Carling has written much more about imaging of adrenal tumors on other sections of this site.
The third step is very important and that is to ask whether the adrenal tumor is cancerous or noncancerous. That is, is it benign or malignant? What do we worry about is either malignant pheochromocytoma or adrenocortical carcinoma if the tumor is cancerous and it is arising from the adrenal gland. Even if the tumor did not originate from the adrenal gland it could be a spread (metastasis) from another cancer INTO the adrenal gland. Again, x-rays, CAT scans, and other x-rays of the adrenal gland can sometimes be helpful. We have an entire section on scans and x-rays for adrenal tumors.
Does the Size of the Adrenal Tumor Matter?
The size of the adrenal tumor is very important for determining whether the tumor is potentially cancerous (malignant), or not. Very small tumors (meaning 1 to 2 cm; less than an inch) are almost never cancerous. However, larger tumors are much more frequently cancerous. As discussed above, any adrenal tumor of any size should be removed if it is making excessive hormones. However, even if the tumor is NOT making too much hormones, tumors that have grown to more than 4 cm in an adult should be removed.Recomendations: we recommend removing any adrenal tumor that is 4 cm (1.75 inch) or larger. For younger patients, we would use a 3 cm (1.25 inch) cutoff. If you have a tumor that is 3 to 4 cm in diameter (1.25 to 1.5 inches in diameter) or larger you probably need adrenal surgery. This is a general guide, and there are exceptions to this rule. This is why it is vitally important for you to seek the advice of experts and especially a surgeon that has EXTENSIVE experience in adrenal gland surgery. This is NOT something to chat about with your local general surgeon that performs gallbladder surgery and hernia operations.
 The large adrenal gland cancer (13.5 cm; arrow) is shown on an MRI scan sitting on top of the left kidney.
The large adrenal gland cancer (13.5 cm; arrow) is shown on an MRI scan sitting on top of the left kidney.
It should be noted that size is not the only criteria for determining whether the tumor is benign or malignant. When we look at the imaging of the adrenal glands, whether it is a CT, MRI, nuclear medicine (MIBG, PET, etc) scan or other imaging study, we need to have a whole-person approach and evaluate all aspects of the tumor and the patient. We carefully analyze the imaging phenotype of the tumor. The imaging phenotype describes all aspects of what the tumor looks like on your scan and helps us determine the likelihood of cancer. It should be noted, however, this is far from a perfect science. In many cases, we can never know for sure whether the tumor is cancerous, or not, short of removing it via surgery.
Experience counts when examining x-rays and scans of adrenal tumors. What we look for on an imaging study (like a CT scan) is a combination of more than a dozen criteria, giving us a total impression, called the "imaging phenotype". For instance, we carefully examine the size and the shape of the tumor. That means we will look at whether the borders are smooth or irregular, whether the margins (edges) are clear or unclear. On a CT scan without contrast, it is important to look at the level of attenuation. Essentially, this is a measure of how dense (or fat-containing) the tumor is based on measurements of what are called Hounsfield Units (HU). The lower the Hounsfield Units (lipid-rich; i.e. fatty) are, the more likely it is not a cancer, but rather a common adrenocortical adenoma. As you can see, it is very important for you to have an experienced adrenal surgeon that has seen hundreds or even thousands of these tumors and their scans so you can get the best treatment.
Adrenal tumors need to be evaluated on a CT scan (with contrast) to see whether the tumor is vascular (has a lot of blood flow or not), or not. Typically, benign adenomas are not vascular, whereas more vascular tumors tend to be either a pheochromocytoma or a malignant tumor. On an MRI, the more intense (vascular) tumors are more likely to be either cancers or pheochromocytomas.
We also look at the presence of necrosis (dying tissue), bleeding (hemorrhage), calcifications (calcium deposits) as well as the growth rate of the tumor in case the patient has had previous imaging of the adrenal glands. Remember that we want to review all your images. Yes, even if you had a scan for unrelated reasons 10 years ago, we want to review it to track the growth of the tumor.
Should the Adrenal Tumor or Adrenal Mass be Biopsied?
NO! A biopsy of the adrenal tumor is almost never helpful and most of the time it can cause significant problems! Important rule: DO NOT PERFORM A BIOPSY OF AN ADRENAL MASS. In fact, it can be very dangerous if the patient has a pheochromocytoma. The biopsy may produce an adrenergic crisis (read about adrenergic crisis in the pheochromocytoma and paraganglioma section of this site). If the patient has an adrenocortical carcinoma (adrenal cancer), the biopsy may spill tumor cells into the surrrounding tissues. The tumor cells can then implant in these nearby tissues and cause local recurrence. Thus sticking needles into an adrenal tumor can decrease the chance of curing the patient, so do not do it. Also, a fine needle biopsy can never distinguish between a benign and malignant adrenocortical tumor, and is thus a wasteful and meaningless, invasive procedure. If your doctor wants to biopsy your adrenal tumor, then please give us a call--you need to seek better advice. The only time to consider a biopsy of an adrenal tumor is if the patient has another cancer, typically of the lung, kidney, breast, colorectal or melanoma and one is suspecting an adrenal metastasis.Because we see this mistake made at least a few times a week, we will say it again: If you doctor sends you for a fine needle biopsy of the adrenal tumor, you need to tell them to read this! DO NOT PERFORM A BIOPSY OF AN ADRENAL MASS.
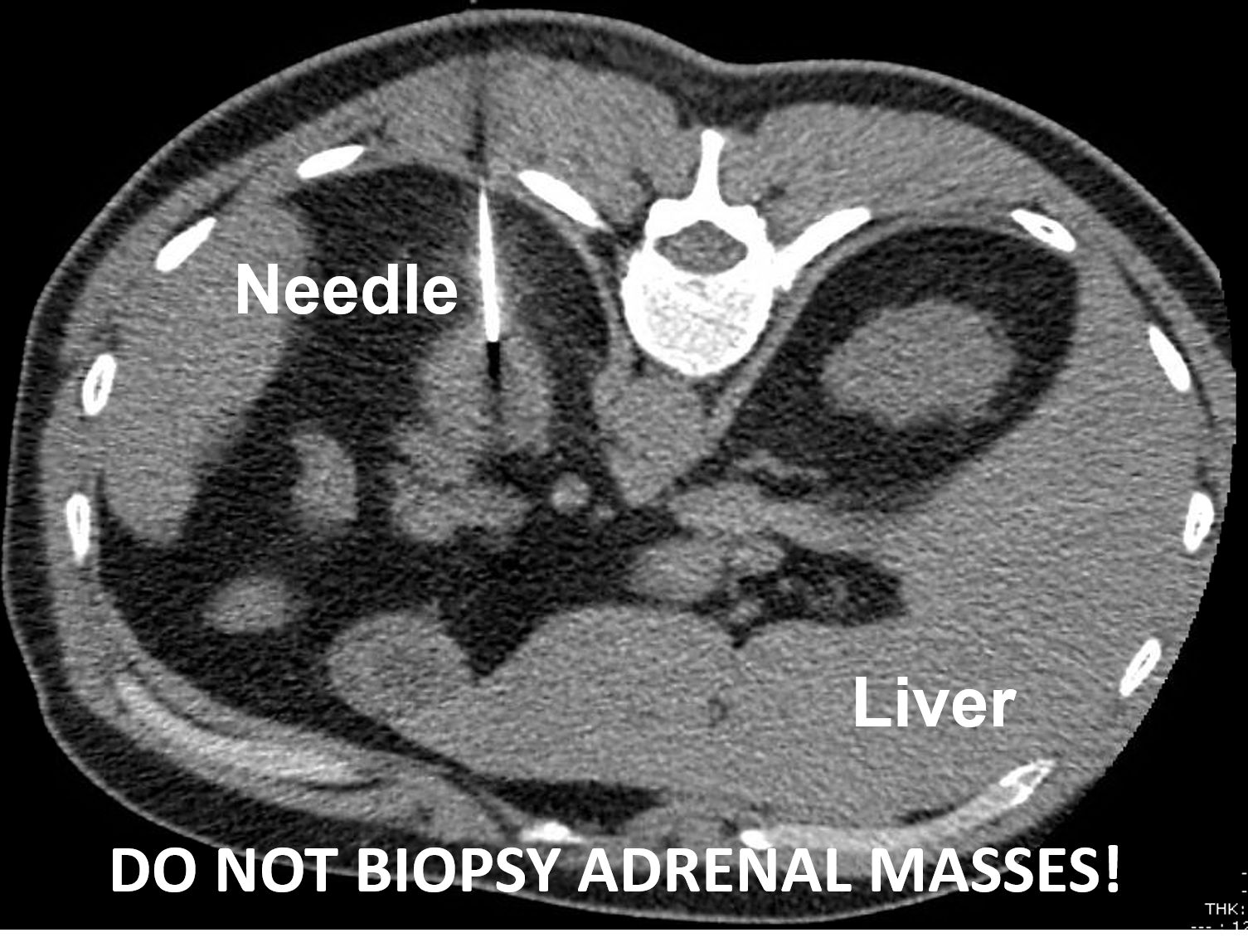 A left adrenocortical cancer undergoing a CT-guided biopsy. This should not be performed. The only time to consider a biopsy of an adrenal tumor is if the patient has another cancer and an adrenal metastasis is suspected.
The rule is to never biopsy an adrenal tumor. As with all rules, though, there are some rare exceptions. The only time to consider a biopsy of an adrenal tumor is if the patient has another cancer, typically of the lung, kidney, breast, colorectal or melanoma and one is suspecting an adrenal metastasis. Now you understand why patients with adrenal tumors should be seen by expert surgeons who have extensive experience with adrenal tumors. It can be somewhat tricky to know in advance of surgery whether the adrenal mass is cancerous, or not. Fortunately, the vast majority of adrenal tumors turn out to be benign. It is important to understand that sometimes surgery (adrenalectomy) is indicated just to prove that the adrenal tumor is not cancerous.
A left adrenocortical cancer undergoing a CT-guided biopsy. This should not be performed. The only time to consider a biopsy of an adrenal tumor is if the patient has another cancer and an adrenal metastasis is suspected.
The rule is to never biopsy an adrenal tumor. As with all rules, though, there are some rare exceptions. The only time to consider a biopsy of an adrenal tumor is if the patient has another cancer, typically of the lung, kidney, breast, colorectal or melanoma and one is suspecting an adrenal metastasis. Now you understand why patients with adrenal tumors should be seen by expert surgeons who have extensive experience with adrenal tumors. It can be somewhat tricky to know in advance of surgery whether the adrenal mass is cancerous, or not. Fortunately, the vast majority of adrenal tumors turn out to be benign. It is important to understand that sometimes surgery (adrenalectomy) is indicated just to prove that the adrenal tumor is not cancerous.
Read about the Mini-Back Scope Adrenalectomy (MBSA), which is the preferred operation for about 95% of people who need adrenal surgery.