Why Is My Blood Pressure So High? I Am Only 40!

Why Is My Blood Pressure So High? I Am Only 40!
You’re 40 years old. You eat reasonably well, you exercise, you don’t smoke, and you’re not carrying a ton of extra weight. Yet your doctor just told you your blood pressure is 160/100—maybe even higher—and it’s not coming down with the usual pills. You feel a mix of frustration and fear. “This is supposed to be something that happens to my parents’ generation, not me.”
I hear this story every single week at the Carling Adrenal Center. And nine times out of ten, the reason isn’t “just stress” or “getting older.” It’s an adrenal gland that has quietly started producing too much of one (or more) of the hormones that control blood pressure and fluid balance. The three most common culprits: primary aldosteronism (PA, also called Conn’s syndrome), mild autonomous cortisol secretion (MACS, or adrenal hypercortisolism; AHC or previously subclinical Cushing syndrome), and pheochromocytoma are far more prevalent than most doctors realize, especially in younger patients with resistant or early-onset hypertension.
Let’s talk about why these conditions strike at 40, how they wreck your blood pressure, what the latest research (including studies we have published) shows, and, most importantly, how expert adrenal surgery can often cure the problem completely.
.png)
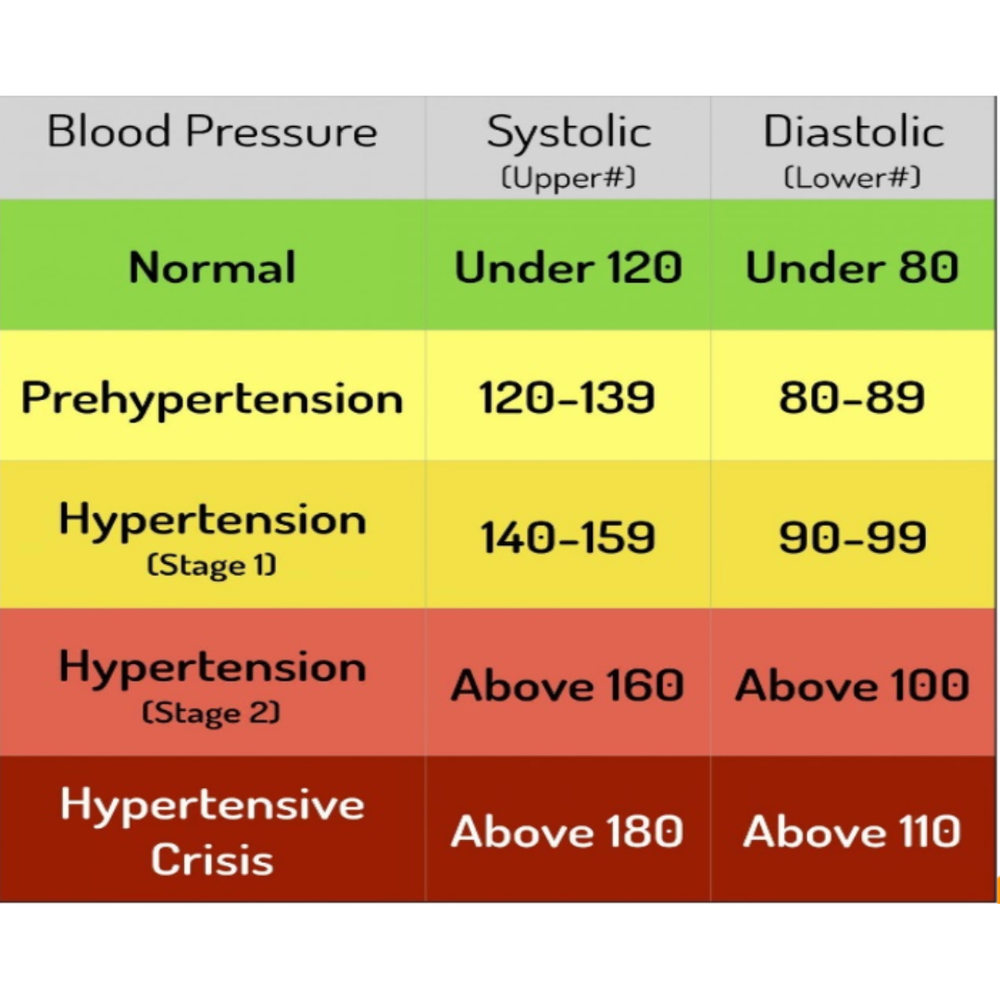
Table 1: High blood pressure categories. Patients with hypertension need to be screened for an adrenal tumor.
The Adrenal Glands: Tiny Organs, Massive Blood-Pressure Control
Sitting on top of each kidney are your two adrenal glands, each about the size of a walnut. They produce aldosterone (which tells your kidneys to hold onto salt and water), cortisol (the stress hormone that also raises blood pressure), and catecholamines (adrenaline and noradrenaline). When one of these hormones runs wild because of a benign tumor or overactive nodule, blood pressure can skyrocket even while you’re still in your 30s or 40s.
Unlike “essential” hypertension—the garden-variety high blood pressure that develops slowly over decades, these adrenal disorders are secondary forms. They have a specific, treatable cause. And because they’re hormonal, they often appear earlier in life and resist standard blood-pressure medications.
Primary Aldosteronism (PA/Conn’s Syndrome): The Most Common, Most Underdiagnosed Culprit
Primary aldosteronism occurs when one or both adrenal glands produce too much aldosterone. The excess hormone makes your body retain sodium and lose potassium, driving blood pressure up and sometimes causing muscle cramps, fatigue, or heart palpitations.
For decades, textbooks claimed PA was rare—maybe 1 % of all hypertension cases. We now know that’s completely wrong. PA accounts for 5–10% of all hypertension and up to 20 % of resistant hypertension (blood pressure that stays high despite three or more medications). In younger patients like you, the numbers are even more striking.
In a 2025 paper I co-authored titled “Primary Aldosteronism: Adrenalectomy Could Save More Lives,” we reviewed the latest data and showed that patients with PA who undergo proper adrenalectomy have dramatically lower rates of heart attack, stroke, atrial fibrillation, and kidney damage compared with those treated with medications alone. The surgery doesn’t just lower blood pressure; it literally saves lives by reversing the hormonal damage before it becomes permanent. Yet fewer than 5 % of patients who should be screened for PA ever get the simple aldosterone-to-renin ratio blood test. That’s why so many 40-year-olds are walking around undiagnosed.
Autonomous Hypercortisolism (AHC): The “Silent” Cortisol Problem
Even more eye-opening is the new data on high cortisol. For years, full-blown Cushing syndrome (with moon face, buffalo hump, and easy bruising) was considered uncommon. But mild autonomous cortisol secretion (adrenal hypercortisolism), where the adrenal gland makes just a little too much cortisol without the classic outward signs, is surprisingly common in people with hard-to-control blood pressure.
In March 2026, the MOMENTUM study, the largest U.S. study of its kind, was published. It screened nearly 1,000 patients with resistant hypertension and found that 27 % had adrenal hypercortisolism. That’s more than one in four! These patients were not the classic Cushing’s cases most doctors look for. They were otherwise healthy-looking 40- and 50-year-olds whose blood pressure simply wouldn’t come down. High cortisol quietly raises blood pressure by increasing vascular stiffness, promoting sodium retention, and messing with insulin and metabolism.
The good news? Once we remove the offending adrenal nodule or tumor, blood pressure often normalizes, and many patients can stop or dramatically reduce their medications. The MOMENTUM results are already changing how endocrinologists and cardiologists screen for adrenal causes.
Pheochromocytoma: The “Adrenaline Bomb” Tumor
Pheochromocytoma (pheo for short) is the rarest of the three but also the most dramatic. These tumors pour out adrenaline and noradrenaline, causing spells of pounding headaches, sweating, racing heart, anxiety, and blood-pressure spikes that can reach 200/110 or higher. Some patients have sustained high blood pressure instead of spells, which is why pheo is often missed in younger adults.
Even though pheochromocytomas are uncommon (roughly 2–8 cases per million people per year), they are responsible for a disproportionate number of hypertensive crises in people under 50. And because the excess catecholamines can damage the heart and blood vessels over time, early diagnosis is critical. The diagnostic test is simple: a blood or urine test for metanephrines. If positive, a CT or MRI almost always finds the tumor, and expert minimally invasive adrenalectomy cures the problem in nearly 100 % of benign cases.
Why Age 40 Is a Red Flag
Essential hypertension rarely appears suddenly at 40 in an otherwise healthy person. When it does, or when blood pressure is resistant to multiple drugs, the odds of an adrenal cause jump dramatically. Genetics play a role—some people inherit mutations that make their adrenal cells more likely to form hormone-producing nodules (we’ve published extensively on the molecular pathways involving potassium and calcium channels in PA and PRKACA mutations in cortisol-producing tumors). Lifestyle still matters, but it can’t explain a 40-year-old with sky-high aldosterone or cortisol.
The Cure Is Often Surgery—Done Right
The best news? For the vast majority of these patients, the mini back scope adrenalectomy (MBSA) is curative. At the Carling Adrenal Center, we perform more adrenal operations than any other hospital in the world, roughly 12–14 % of all adrenalectomies in the USA. We use individualized, tailored approaches: partial adrenalectomy when appropriate to preserve normal adrenal tissue, precise vein sampling for complex PA cases, and early discharge for >99.8% of patients.
My patients routinely tell me their blood pressure normalizes within days to weeks, they feel energy they hadn’t realized was missing, and they get their lives back.
What Should You Do If You’re 40 with High Blood Pressure?
- Ask your doctor for an aldosterone-renin ratio blood test (the screening for PA). Look at both results carefully. Nothing other than PA will cause a very low renin level. Pay attention to the renin level, not only the aldosterone level!
- If you’re on blood-pressure medications and still not at goal, ask about a 1-mg dexamethasone suppression test to screen for too much cortisol secretion. This test, together with ACTH and DHEAs levels, clinches the diagnosis of adrenal hypercortisolism (MACS)
- If you have spells of anxiety, sweating, or labile blood pressure, request plasma-free metanephrines.
- If any test is positive, get referred to an adrenal center that does high-volume adrenal surgery
Don’t settle for “it’s just high blood pressure.” At 40, you have decades ahead of you. Finding and fixing an adrenal cause can prevent heart disease, stroke, kidney failure, and a lifetime of pills.
If you or someone you love is in this situation, we’re here. The Carling Adrenal Center in Tampa, Florida, is the national and international destination for patients with adrenal tumors causing hypertension. We see patients from every state and >50 countries because the difference between “living with high blood pressure” and “being cured” is often just one correct diagnosis and one expertly performed operation.
You don’t have to accept high blood pressure at 40. Let’s find out why it’s high—and fix it.
Have questions? Reach out to us at the Carling Adrenal Center. We’re here to help you get answers and get back to living your best life.
Dr. Tobias Carling, of the Carling Adrenal Center, is one of the world's leading experts in adrenal gland surgery. Dr. Carling performs more adrenal operations than any other surgeon in America. Dr. Carling left Yale University in 2020 to open the Carling Adrenal Center in Tampa, Florida.
To discuss the details of your case with Dr. Carling and become his patient, fill out the new patient form, and he will be in touch with you shortly.
Additional Resources:
- Learn more about the Carling Adrenal Center
- Learn more about Dr. Tobias Carling
- Learn more about our sister surgeons at the Norman Parathyroid Center and Clayman Thyroid Center.
- Learn more about the Hospital for Endocrine Surgery
- Read about high blood pressure, parathyroid disease, and hyperparathyroidism here
- Changes in your blood pressure can also be related to thyroid disease. Read about thyroid disease, hyperthyroidism, and thyroid surgery here